On Monday, as scheduled after radiation, I went in for PEG placement. Although I can still eat, it’s highly likely that due to the treatments I am receiving to my mouth and throat, I will become unable to eat at some point. Hence, a feeding tube is necessary, preferably before it actually becomes necessary. So, off we went to the GE (gastroenterological) Lab at the hospital for a bit of outptient surgery.
The lab is very, very cold. Even one of the nurses was complaining about it, which is rare, since just about every medical place you go feels like a meat locker. They gave me some fluids, then took me back for anesthesia. I had not eaten since Sunday night, and had no liquids since 8 AM. I was, therefore, quite hungry and very tired.
The anesthesiologist introduced himself, and said he would be giving me something to make me sleepy. I told him I was already sleepy. So he told me, ok, we’ll give you something to make you sleepier. Fine by me, I said, as long as I sleep through the whole thing. No problem.
The process, they explained, was pretty simple. They stuff a scope down my throat and look for an appropriate place to place the tube. Once they found it, they would do a little laproscopic procedure to insert the tube into my stomach and secure it inside with a small balloon. The entire procedure takes about 20 minutes or so.
Thye knocked me out, and the next thing I knew, I’m in recovery, with a tube sticking out of my gut. The papers said there may be some “slight discomfort” due to the incision and to the gas (air) they pump into you while they place the tube. Slight was a bit of an understatement.
What they did not give us was any instructions on actually using the thing, no syringes, and nothing for pain. The latter was the most important thing, as you’ll come to see soon.
After another 20 minutes or so, they let me go home. Mom took me back to her place, where I promptly aid down and tried to get a little rest. Alas, this was not to be. I had a few sips of Gatorade and water, and fell asleep for a few minutes. Half an hour later, I was throwing it up again. We tried again, this time wih water only, plus some Motrin for the pain that was rolling through my gut. That came back up as well.
By this time, the pain was beginning to be severe, with spasms rolling up through the incision area, causing me to actually cry out in pain. At some point, I finally drifted off again, only to wake up with even worse pain. I mumbled to my family that I didn’t think it was supposed to be this way, and please call the doctor’s office.
They did just that. The doctor called back, and told them to take me to the nearest ER for a contrast xray, to ensure the tube hadn’t been displaced by the vomiting.
No, not that kind of drinking, you lushes. I’ve never been much of a drinker, as just about anyone could tell you, and haven’t had a drop of alcohol since I was diagnosed, strangely enough. It did occur to me on that day to go out and get blasted, but that sort of thing doesn’t appeal to me when I’m in good health anyway, and the sane part of my cranium took over.
So what are we drinking?
Boost, nasty chocolate-flavored, vegetable-oil filled, high calorie, no fiber, high protein drink. Sip. Water. Sip. Swallow together. It’s really the only way to get the stuff down, and has become my morning meal. Not because I can’t eat, precisely, but because it takes me so long to eat and my schedule has changed, that I would be tired out before leaving the house, just from shoving down whatever real food I may have.
And why, you may ask, has the schedule changed? Amifostene, mentioned earlier. I now have to go to radiation 30 minutes before my actual scheduled time to get two shots in the ab area (subcutaneous, for those following the technical bouncing ball). It doesn’t hurt so much – yet – as it burns when the drug goes in. Since I have to get two a day before every treatment, I’m certain that at some point my abs will feel as much like a pincushion as the rest of me is.
Since Sprint has finally kindly cooperated and allowed logins once more (they were revamping due to the merger with Nextel), here are a couple of pics for you. Icky medical stuff, so if you don’t like it, don’t look.
Last week, as you may recall, I headed over for the loading dose of the program drug (erbitux).
I didn’t have any of the severe reactions to the drug, like shortness of breath, difficulty breathing, or death. What I did get the next day was the horrible flu-like symptoms. On Friday, though, I got one of the most common reactions: rash. It’s an acne-like rash that really looks like you’ve just entered puberty and the fun hormonal stuff that goes with it – although I have to say I never had anything this bad at any age. On the face, it really just looks like a horrid case of acne. I’ll post an image of that later – for lovers of b-grade horror flicks, it looks like pustules on a zombie. Or the plague.
Everywhere else, it looks more like chicken pox, although you can still see the acne-like stuff up close. I’ll post pics of that as well.
It has gotten progressively worse since then, and is appearing in various degrees on just about every part of my body. The upside: there is a cream they can prescribe to try and keep it in check so you don’t look like one big pimple, as Rita puts it. Unfortunately, virtually no pharmacy carries it, so it has to be special ordered.
This week, starting on Tuesday, we began in earnest with the full treatment.
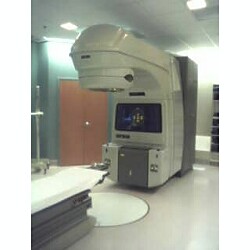
Tuesday was measurement day, wearing the Mask of Doom. The outside room, where the radiologists are, is quite high tech. Computers control positioning, dosing, movement of the machine, and there are a couple of monitors looking down directly at the patient at all times. The techs also have an intercom so they can talkto you while you’re locked down on the table. I asked Peggy (the radiology tech on duty Tuesday) if I could take a picture of the machine – a linear accelerator, for those into technical terms – and she said go right ahead. So I did.
The headrest you see has locks around it. This is where they lock the mask down over your head and shoulders to keep your head from separating itself from the rest of you. Or at least to keep it still.
Peggy took all the measurements and then took a couple of xrays so the doctor could verify exactly where they wanted the beams to go based on the fact that I am currently cancer-free and this is more of an aggressive preventative thing than anything else. The entire process for this actually took longer than a regular treatment takes, due to all the moving, marking on the mask, shifting, etc. Xanax, however, is my friend. I’m going to try to get my mom to take a shot of me locked down to the table on Thursday, just so people can see what it’s like. Treatments will run about 10 minutes in total on days where they don’t need to adjust anything or take more film.
Wednesday, it was back to chemo. I learned my lesson the first time around, and this time was dressed more appropriately in sweat pants and had a flannel shirt with me. First, the Benadryl, to offset any reactions to the erbitux. Then a thirty minute break while I tried to stay awake and realized that large doses of Benadryl make me have to go to the bathroom. I got Rita to unhook me so I could stumble off and do my thing while we waited. Next up: erbitux. Takes about an hour or so to drip in. Change of bags to anti-nausea drugs to offset the potential for puking from the Taxotere. Another 30 minutes for that. Then, on to the Taxotere, which took another hour or so. All told, we got there at 10 AM for our appointment, didn’t actually start the chemo until 11:30, and finally got out of there just before 2:30. The radiation appointment on Wednesdays is at 2:45. Luckily, the outpatient cancer center is right down the road from the main hospital complex, so we scooted over.
I had tossed a Xanax back shortly before we finished up with the Taxotere. Between the Benadryl, the antinausea stuff, and that, I was pretty mellowed out and ready to go to sleep when Peggy took me back to the treatment area. I took off my shirt and put on a gown, and got locked in without too much panic bubbling up at all.
I got myself zapped form the right side, the left, and then straight on, with one more xray taken at the end from the straight down view. And then, it was done. I had so many drugs in me, I think I must have dozed out for a few seconds toward the end. Next thing I knew, Peggy is snapping me out of the Mask of Doom and I’m on my way to talk to the doctor and look at my PET/CAT scans. Those were absolutely some of the most amazing things I’ve ever seen. Both scans were done with contrast. On the PET scan of my mouth, the tumor on my tongue is lit up as bright, bright red-yellow-orange in a sea of dark. The left throat also shows the nodes that were affected in that bright color. If I had a scanner, I’d ask for copies to scan and post just so people could see how cool they are.
And that was that. Off to the NOC to rack up another four servers, with one more in the pipeline, then home. Thursday, it will be time for more radiation – in fact, every weekday will be radiation, every Wednesday will be chemo plus radiation afterwards. So my schedule it set for the next seven weeks.
One note about something else that tells me how screwed up things can be. There is a drug called amifostene that is used to help retain salivary function in people who are undergoing radiation treatment to the head and neck. This is important, since when you think about it, your saliva is part of what helps you fight off cavities and other mouth-related nastiness. The doctor recommended it, it’s not forbidden on the study I’m in, so we said absolutely.
It’s an injection drug, and it’s $500. Per injection. You have to have it before each treatment. So, for 35 treatments, that drug costs over $17,0000. It’s amazing that anyone can afford any quality medical care if they have no insurance. Fortunately for me, the folks at the hospital got me into a program since I’m on this study and have no insurance, so it’s unlikely I’ll have to pay for any of that. Good thing, too, with the rest of the bills piling up. But, again fortunately, I don’t think I could have asked for a better group of people to be handling my care than those we’ve found here. They’ve all been fantastic.
Wednesday was the final visit to the ENT who performed my surgery before we get into the fun and games of chemo and radiation. It all looks good, of course, and the swelling, although still severe, will go away eventually. That’s good news for me, even though I wonder how much of that will be in the next 6-7 weeks while I’m wearing the Mask of Doom every weekday. The horizontal incision is almost completely closed, and this next week will be the end of healing for that until a few weeks after treatment ends – radiation and chemo kill healthy cells, too, so healing in the area will cease until my body recovers a bit from the treatments. I’ve resigned myself to having it not heal all the way before we begin, as there are certain time constraints we have to deal with, both for the study of which I am now a part and for general purposes, since they recommend post-op treatment within a certain period of time.
I told the doctor that the incisions burn from time to time, like a fireline lit up along each. That’s actually a good thing, since it means the nerves are attempting to repair. Of course, that healing will be destroyed by what we’r about to do, but it, like the general wound healing, will restart as we shake through the weeks following cessation of treatment.
So what poison am I referring to? The chemo drugs, of course. Wednesday directly after the ENT visit, we jumped across the bridge and went in for the first round (the loading dose). To start, Rita (the oncology nurse handling me there) put in an IV. Not in the crook of my arm where the nice big veins are, but in my forearm. This is because the first treatment was going to take about two hours or so, and the remaining treatments will take about three hours each. As she pointed out, not being able to bend your arm during all that time would be pretty lousy. It wasn’t as painful as I thought it might be, and of course, unlike some of the other people there receiving treatment (all women, interesting), I don’t have to wear my IV all the time. Several of the women had catheters (caths) in their chests where they received their drugs. Those are inserted for people who get chemo on a daily basis for whatever ailments they have.
The first bag hung on my IV was benadryl. This is to control some of the potential side effects of the experimental drug. They are more lke allergic reactions than anything else, as with any drug: hives, rash, a feeling of tightness in the throat, trouble breathing. There was so much benadryl in the bag, though, and I was so tired from having been up all day and night and into Wednesday morning dealing with the aftereffects of a DOS attack to one of our clients, that about five minutes after she hung the bag and was explaining some things to my mother and me, I could feel the sleep trying to overtake me. Apparently, my face flushed pretty badly at one point, and I could feel the heat of that, but it subsided. Once that bag was done, we waited 30 minutes and Rita hung the bag with the C225 (erbitux). I kept dozing in and out while it dripped along for an hour or so. I didn’t feel any particular side effects, and whether that’s due to my general health (exceppent except for the whole cancer thing) or due to the bendaryl is anyone’s guess.
When that had dripped out, I had to stay for another hour so they could monitor me for any reactions or problems. There were none, so they kicked me out.
It’s cold in the treatment room, and I was curled up in a blanket when my mom came back in – she had gone off in search of something to eat. But I noticed that even when we left, I was cold. As soon as we got back to her house, I changed into my sweats and wrapped myself in a blanket. Since the blanket was hard to keep on and still do the work I needed to do, my mom dug out a flannel shirt for me. Picture this: it’s about 92 or so here during the day, on average, during the summer. I’m bundled up like it’s 20 degrees outside. One of the potential side effects after treatment is flu-like symptoms: headache, chills, low grade fever, muscle achiness, etc. These should subside the further you get from the dosing. My head is killing me, and I’m chalking that and the chill up to a minor side effect of the dosing. Next week, I will get the C225 plus antinausea drugs and the regular chemo drug, Taxotere, since I was randomized into that group. That same combo will be given for the next six weeks, every Wednesday morning before I head over for that day’s radiation.
The clinical research nurse (Jan) gave me a great calendar with all my events: daily radiation, weekly chemo, weekly blood work, and a note that CAT scans may be ordered during the treatment phase if they think they need one. I’m guessing that as we really get into it, I won’t care what they want to do any longer. We begin radiation on Sept. 6 and the radiation oncologist says the side effects of that will begin to appear pretty rapidly after we start: fatigue, sunburn-like patches on my face and neck, dryness of the mouth, mouth sores, thick mucous in my mouth – all of these are potential side effects, with some, like the fatigue and sunburn, unavoidable, and others, like the mouth sores and thick mucous, potentially mitigated by certain drugs and activities, like oral rinses. We shall see. One of the possible sie effects of the chemo is hair loss, although they tell me with my dosage only once per week, thinning is more likely than total loss. I told them that Stacy promised to find me some colorful and fun ‘do rags if hair loss crept into the picture.
What now? Not much: continuing to work, of course. The college football season officially starts tomorrow (today, I guess, since even though this post started on Aug. 31, it is being posted on Sept. 1), and the pro season follows next Thursday, so it will be a lot of football and FoodTV for me in the coming two months. That would be usual, too, for my viewing habits, so I guess you could say that the treatment won’t affect certain of my habits all that much.
Shout out to those of you who may have been affected by Katrina. I know you’ll get through it, just as people always do. Survive a tragic event and then move on and continue to live. It’s the only way to go.
Monday morning I headed to the slab for a dry run. They do simulations, with everything just as it would be for radiation, except without the radiation. This means lying down on the bench, snapping on the mask, and the radiology techs making marks on the mask so the beams can be aligned.
Not fun.
Since the left side of my face is pretty swollen still, the mask is even tighter than it was the first time around. In addition, it now pressed right on the tip of my nose and across my brow more tightly than before. I got the tech to cut out a smal portion around my brow, but they really can’t do that with the nose portion, since that’s what presses me into the table and keeps me still vertically. That’s disappointing, because I can’t open my eyes in the mask now, either, which means I’m just lying there, blind, whie they do their thing. On the plus side, I had swallowed down one of the Xanax prescribed to me, and my panic wasn’t nearly what it had been with the PET scan, although it was still pretty bad. Between the nerves and the (re)fitting, it took four tries to get the mask in place. Once in place, though, that Xanax started kicking in a bit more, and I patiently waited for the techs to do their thing. The procedure itself took about five minutes or so, and they told me that typically it will only take that long for each treatment. They schedule patients 15 minutes apart, so as long as they can get someone in place in a reasonable amount of time – or get the mask on them without them hyperventilating into a heart attack – they can get a lot of people in and out through the day. I have enough drugs plus refills to last through the treatment period of 6-7 weeks, so I think I can do this.
Tuesday, it’s off to the dentist, to make sure that I don’t need any major dental work before we begin. I’m sure I don’t, but I also have to pick up flouride trays to use throughout treatment so all my teeth don’t fall out, so it’s a necessary stop.
Wednesday, it’s off to the surgeon so he can check out his handiwork again. I fully expect him to give the all clear, even though the horizontal incision is not completely closed, and Wednesday afternoon, it’s off to the medical oncologist for the first round of chemo. That visit will take about an hour and a half or so, as it’s the loading dose of the drugs I’ll be receiving once per week for the next 6-7 weeks. Subsequent visits will be in the range of about 3 hours a pop.
As I expected, the first round of radiation will be on Sept. 6 – the day after Labor Day – and will be every weekday for the entirety of the treatment period. Things should start getting interesting pretty quickly, given the effects radiation and chemo have on the body. I can’t wait for it to be over, and we haven’t even started!
I now have a date with a tube. A feeding tube, that is. On the 19th, I will be the proud recipient of a tube that will help me reach certain goals, like staying nourished in order to stay alive through treatment.
Last Thursday, we met with the dietician and then the radiation oncologist.
I’m not having any particular issues eating at the moment – that is, I can get food down, although it takes me awhile to do it. There are very few things I really can’t eat at all. Bread is one of those things, which is too bad, since I really like fresh bread. It’s simply too dry and takes too much water for me to work my way through a single slice. Anything else is pretty much fair game as long as there isn’t too much of a skin on it, as that gets caught on the roof of my mouth and I either have to fish it out with my fingers, which disturbs whoever I’m eating with, or I have to swish some water around in my mouth, which often just works to move the stuck piece to another place in my mouth where I can no longer move my tongue to get it down, resulting in me having to reach in again.
Anyway, back to the dietician. She did ask me about my eating habits, and at my weigh-in, I was at about the same weight I had been the week before at the surgeon’s office, so I guess my weight regain is slowing down. She did the calculations, and to maintain my current weight during treatment – especially when we really start going into the heart of it – I’ll have to take in 2200 calories a day. “How many calories is that again?” I asked. I don’t think I’ve ever eaten that many calories in a day. Fortunately, there are all sorts of liquid meals available to provide calories and nutrients. The dietician also showed me one item I thought was amazing: it’s a little tub, 1.5 ounces (yes, ounces) of a colorless, tasteless liquid. That little tub has 330 calories by itself. Amazing what modern science can do.
The radiation oncologist had a look at my neck, said it looks good (and it does), and that we should get the all clear from the surgeon and get going. He also wanted to schedule the sim(ulation) for that day, but their machine was down, so it was rescheduled for Monday. The clinical research nurse came in and I signed off on the consent forms for the study, then headed upstairs so the lab could draw some blood for a baseline workup before starting treatment. It’s a little nervewracking to know we’re very close to beginning the next phase.
On Tuesday, we saw the medical oncologist for the first time. While going through the standard questioning about my symptoms and surgery, the doctor asks, “So, you don’t smoke, never have, don’t use tobacco products, and don’t live in a house where others are smoking. How’d you get cancer?”
Beats me, doc, I thought that’s what the guys and gals in the white lab coats were supposed to figure out.
Nice guy, though, and we talked about this clinical study the radiation oncologist said I would qualify for. The medical oncologist is pretty sure this new drug will be approved for head and neck cancer very soon, just as it is approved now for advanced colorectal cancer. The bonus is that of course the manufacturer would pay for the new drug, and depending on which group I land in (that is, which of the chemo drugs I’d get in conjunction with it), they would pay for one of those drugs as well. In his estimate, the cost for the experimental drug itself would run just shy of $100K for a year’s worth of treatment. So, from both a medical and an economic standpoint, he said if he were in my shoes, he’d go ahead with the study. It’s not going to do any harm, and the efficacy is good either way, so there you go.
He also recommended that I go ahead and get fitted with a feeding tube before the treatments start. There are quite a few side effects associated with receiving radiation to the mouth and throat, and having chemo at the same time can make those side effects a bit worse: sores in the mouth, trouble swallowing, painful swallowing, loss of appetite (which would be complicated by the pain in the mouth), etc. Getting the tube in before treatment starts would be much better than getting the tube when things start getting too painful, of course. What they do is run a tube down your throat, make a small incision in the abdomen, and pull the tube out. Then you just uncap it, pour in whatever it is you’re drinking, and put it away. So we decided to go ahead and do that. I’ll eat regularly as long as possible, and then if I need it, it will be there. Now we have to wait for the referral to the gastroenterologist, who will do the procedure.
On Wednesday, we saw the ENT once more. He removed the dressing, scrubbed out the open incision with some gauze and peroxide, and pronounced the wound as “looking very good”. And so it is: on my right side, under my chin, the incision has closed up again entirely, and the big hole on my left where the two incisions meet is down to between 1/4 and 1/2 inch deep. It’s a little weepy, of course, but that’s healing for you, and it’s not the same smelly, nasty weeping that was the reason he ripped it open again in the first place. The best part is that it no longer needs to be dressed. The remainder of the heaing can be done in the open air, although I still have to be very careful not to get anything into the wound.
One funny exchange: my mom took my to this appointment, as she has to all the others. When the doctor indicated the dressing would not have to be replaced (great news for me, since the constant gauze and tape were highly annoying and irritating on my neck), she asked if I could shower now (rather than taking a bath, which is what I had been doing). His reply, with a sort of fake relief:
“Oh, yes, please do.”
Funny guy. We like him quite a bit.
And I have to tell you, I love showers. I’ll take a shower over a bath any day, and particularly now, since showering takes a lot less energy than bathing. It also means I will no longer need to kneel on my hand and knees and stick my head under the faucet in order to (carefully) wash my hair while trying to keep the dressing around my neck as dry as possible. No way, baby: now it’s a sort of contortionist bend backward to let the water run over my head. I’m still unable to raise my left arm all the way over my head, so I have to tilt my head down and to the left if I want to use my left hand to wash the old mop. Still, it beats the alternative.
The numbness continues to recede down the left side of my face. I can actually feel most of my cheek now, except from directly below my left cheekbone down to my jaw and across my jaw to my chin. My ear is still numb, but strangely enough, I can now feel the inside of my ear, in the ear canal. Behind my ear, down my neck, and into my left chest is still numb, alas, and the left side of my face is still significantly swollen. I look a bit lopsided, to tell the truth. One really annoying thing is that my left neck and chest are just hard to the touch – I can’t feel anything but the pressure, of course, but I can feel with my fingers that the area is much like pressing on the surface of a table: fairly unyielding. To get an idea of what it’s like, press gently on the front of your neck somewhere, on either side of your windpipe. Feel that give? Now, using the same gentleness, press down on your countertop or your table. The latter is what my neck feels like. The doctor assures me that will get better and is a result of the stuff they removed. I’ve also found that I’m starting to get itches in my neck, shoulder, and chest where the numbness is. The problem? They’re on the inside. I can’t feel myelf scratching my skin in those areas, and pressing too hard hurts, so I’m stuck with these nerves waking up, apparently, and no way to do anything about it. It’s difficult to put ice or heat on it, since too much pressure hurts, and there’s also a bit of danger there, since I can’t actually feel anything, and something too hot or too cold could damage the skin or tissue and I’d have no idea it was happening. I just squirm a bit until it goes away for now.
This week, we’re back to the radiation oncologist, where we’ll probably be setting a date to begin treatment. My guess? After Labor Day. The wound should be healed by then. Then we get to deal with what they’re going to do with me, and I am not looking forward to that at all. The thought of the mask is giving me nightmares…
I should have had insurance at the end of 2004. Between an agent who was impossible to get hold of and a company who couldn’t seem to get my records from my doctor’s office in a timely manner (they claimed they never got them, the doctor’s office says their records show they were in fact sent), the policy that I had signed up for was vacated. Naturally, while we were trying to figure out what was going on and trying to find alternate coverage, so as not to deal with the Agent From Hell (AFH), I was diagnosed with cancer.
Ha, ha, say the corporate overlords who run the insurance companies. No insurance for you! Pre-existing condition! Neener, neener.
No one actually said that, of course, because as soon as the biopsies came back, I knew I was going to foot the bills and I didn’t have the patience to listen to anything like that.
I’ve not yet received a bill from the hospital, but apparently while I was completely out of it the first day, a very nice lady from the financial office stopped in and had a chat with my mom. She also brought along the printout from the first day’s festivities: about $15,000. That would be for the surgical stuff, staff, room, whatever drugs they pumped into me, and so on. I’m sure the following days weren’t billed at that particular rate, but we’re still waiting for their accounting to catch up.
My ENT’s office called me, and then sent a nice letter with his total: just shy of $8,000.
And some of the others:
PET scan: $4,000.
CAT scan: $2,000.
Radiation oncologist: $5,000.
Medical oncologist: $5,193.
Radiologists: $600.
Pathologists: $300 .
There’s more, but you get the idea. I have to say, though, that everyone we’ve dealt with has just been great. The first medical oncologist the radiation folks tried to get me into wouldn’t even take self-pay patients. The second one did, and as an added bonus, the doctor agreed to shave 50% off the total bill, which is why that’s such an exact number up there. They also wanted half up front, either by credit card or cashier’s check, because as the nice woman in his office said (and not in an offensive way, of course), they’d been burned by people not paying or bouncing checks or what have you. I told her I understood perfectly, since I run a business too, and I would happily give them what they asked for in return for their generosity. This is not to say that it’s possible for me to do this for all of these fine people, but hey, I’m alive, and they’re all very understanding that it’s going to take some time to get them what they have due.
If you have the opportunity, do yourself a favor and get health insurance coverage, even if it’s catastrophic insurance at a minimum. If you never need it, more power to you. That’s the best possible scenario you could get. If you do need it, you’ll be happy you had it.